
Abstract
Background: Rehabilitation of severely atrophic jaws remains challenging, particularly in elderly patients with limited bone volume and unfavorable anatomical conditions.
Case presentation: A 75-year-old female patient presented with a fully edentulous maxilla affected by Kelly syndrome, advanced maxillary sinus pneumatization, and reduced bone height and width. The mandible showed an anteriorly positioned inferior alveolar nerve in the premolar regions. Full-arch rehabilitation was performed using an All-on-Six protocol in the maxilla with six straight MegaGen BlueDiamond® implants (Ø 3.3, 3.7, and 4.1 mm) placed using a palatal approach and osseodensification with Densah® burs. The mandible was rehabilitated with an All-on-4 protocol using MegaGen AnyRidge® implants (Ø 3.5 and 4.0 mm).
Results: All implants achieved insertion torque values above 40 Ncm, providing excellent primary stability despite compromised bone conditions. Healing was uneventful, with no biological or neurosensory complications.
Conclusion: The combination of a palatal approach and osseodensification may represent a predictable and minimally invasive alternative for full-arch rehabilitation in atrophic jaws.
Keywords: Dental implants; All-on-4; All-on-6; Palatal approach; Osseodensification; Densah burs.
Introduction
Severe alveolar ridge resorption in edentulous patients represents a major limitation for implant placement, particularly in the posterior maxilla where low bone density and sinus pneumatization are frequently observed. Traditional solutions often involve sinus floor elevation or extensive grafting procedures, which may increase morbidity, treatment time, and cost, especially in elderly patients.
In recent years, full-arch implant-supported fixed prostheses using concepts such as Allon-4 and All-on-6 have become well-documented alternatives for the rehabilitation of edentulous jaws. The success of these protocols depends largely on achieving sufficient primary implant stability, particularly when immediate loading is planned.
Osseodensification is a non-subtractive drilling technique introduced to improve bone density around the implant osteotomy by compacting autogenous bone rather than removing it. The Densah® burs system (Versah®, USA) has been shown to increase peri-implant bone density, enhance implant stability, and improve bone-to-implant contact, particularly in low-density bone.


Case Presentation
Patient Information
- Age: 75 years
- Sex: Female
- Medical History: Non-contributory
- Dental History: Long-standing maxillary edentulism and progressive mandibular tooth loss
Clinical and Radiographic Findings
The patient presented with complete edentulism of the maxilla associated with Kelly syndrome, characterized by advanced anterior ridge resorption and flabby tissue.
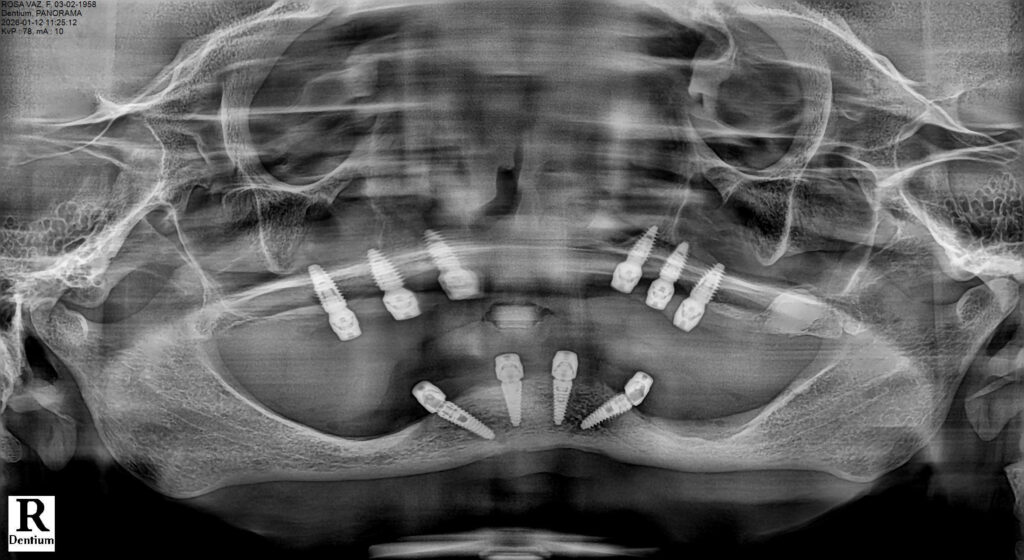
Radiographic evaluation revealed severe pneumatization of the maxillary sinuses and limited residual bone height and width. In the mandible, the inferior alveolar nerve was located in the region of the first premolars, restricting posterior implant placement.
Treatment Planning
Maxilla
- Protocol: All-on-6
- Implant System: MegaGen BlueDiamond®
- Implant Diameters: Ø 3.3 mm, Ø 3.7 mm, Ø 4.1 mm
- Implant Configuration: Six straight implants placed between the maxillary sinuses
- Osteotomy Preparation: Osseodensification using Densah® burs (Versah®)
Mandible
- Protocol: All-on-4
- Implant System: MegaGen AnyRidge®
- Implant Diameters: Ø 3.5 mm and Ø 4.0 mm
- Implant Configuration: Four implants placed anterior to the mental foramina
Immediate loading with fixed provisional prostheses was planned for both arches.
Surgical Procedure
Pre-surgical Planning
A comprehensive diagnostic work-up was performed, including panoramic radiography and cone-beam computed tomography (CBCT), to assess bone volume, sinus pneumatization, ridge morphology, and the position of critical anatomical structures.
The maxillary arch presented severe horizontal and vertical bone resorption, advanced sinus pneumatization, and a palatal shift of the residual ridge, consistent with Kelly syndrome. In the mandible, CBCT analysis revealed an anteriorly positioned inferior alveolar nerve in the premolar regions, limiting the safe placement of implants in these areas.
Based on these findings, a full-arch rehabilitation was planned using a fixed implantsupported prosthesis, with an All-on-Six protocol in the maxilla and an All-on-4 protocol in the mandible. Implant diameters and lengths were selected to maximize primary stability while respecting the available bone volume and avoiding the need for extensive grafting procedures.


Palatal Approach for Maxillary Implant Placement
Due to the severe horizontal bone deficiency in the maxillary crest, implant placement using a conventional crestal approach would have resulted in buccal fenestrations or dehiscences. Therefore, a palatal approach was intentionally adopted for all six maxillary implants. This technique involves positioning the implants slightly palatal to the prosthetically ideal crest, engaging the denser palatal cortical bone and the basal bone of the maxilla.
The palatal approach offers several biomechanical and biological advantages in atrophic maxillae. The palatal cortical plate typically presents higher bone density compared to the buccal aspect, allowing improved primary stability. In addition, this approach reduces the risk of buccal bone loss and soft tissue recession, which are common complications when implants are placed too buccally in resorbed ridges. From a prosthetic perspective, palatal positioning enables a more favorable emergence profile and reduces cantilever forces on the buccal aspect of the prosthesis.
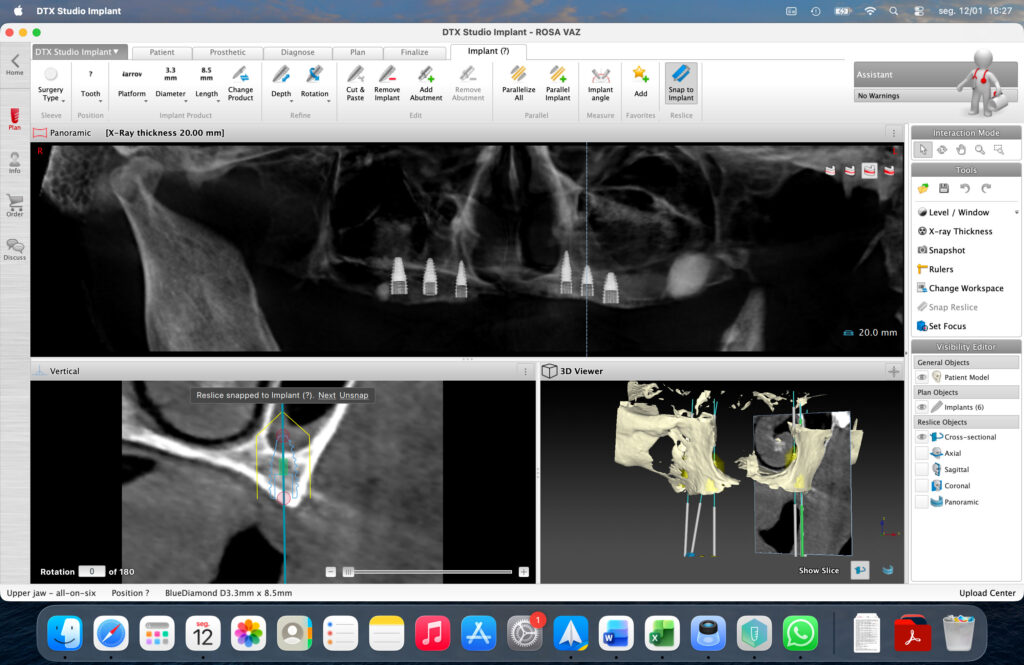
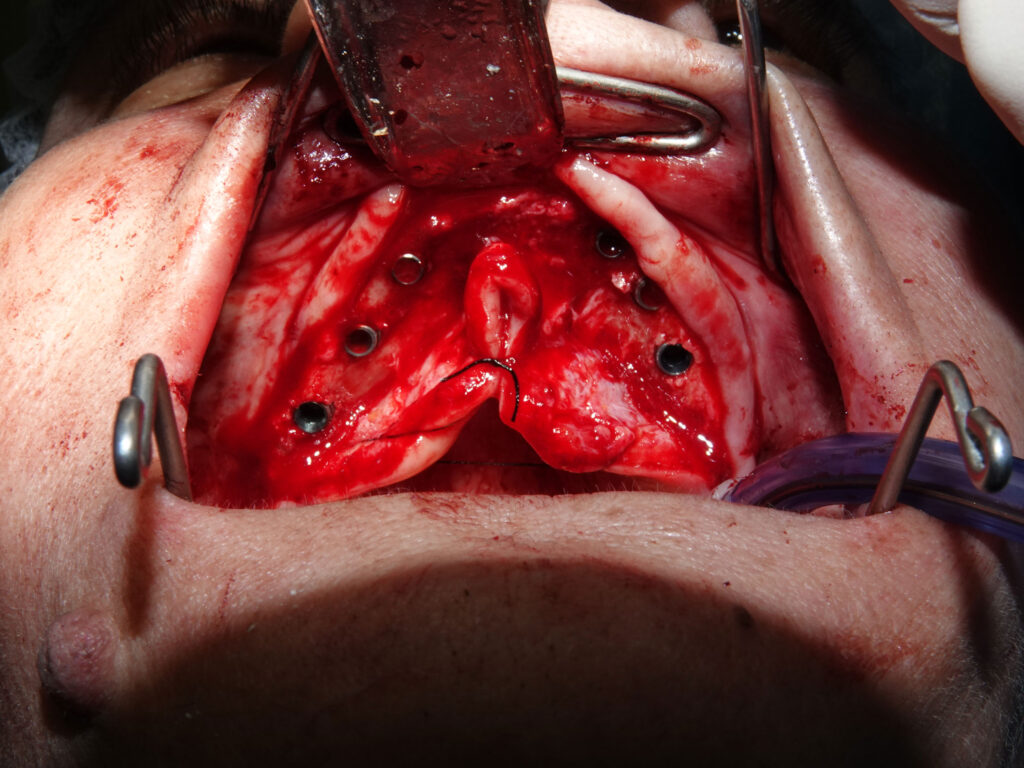
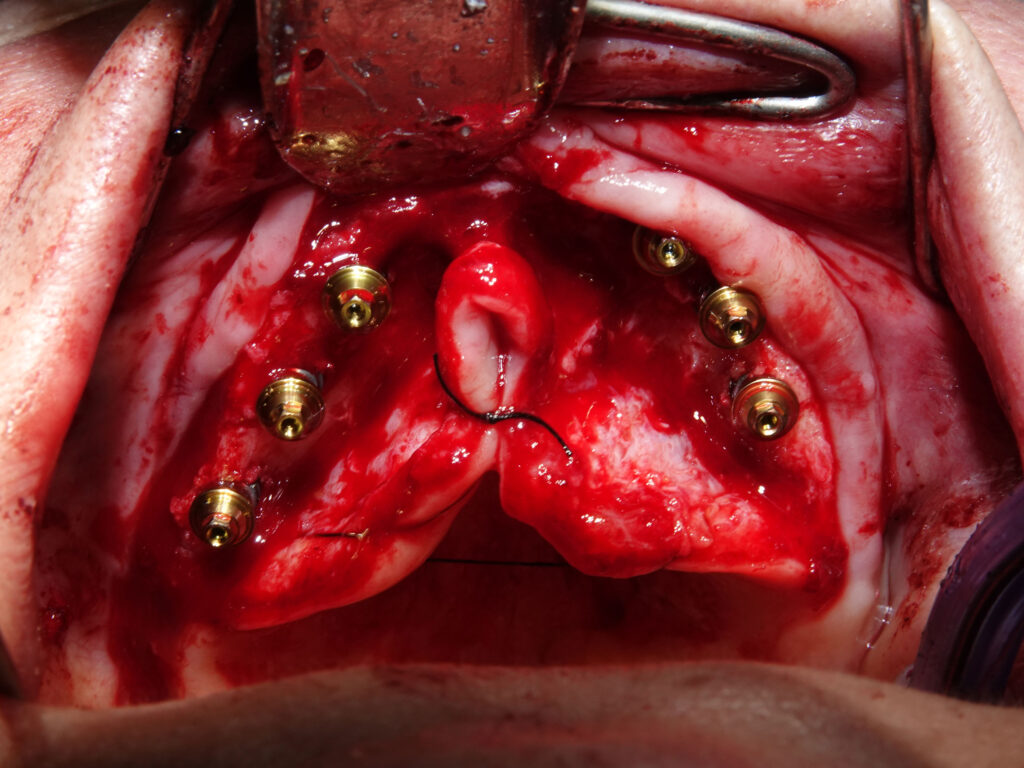
A full-thickness mucoperiosteal flap was elevated with careful preservation of the palatal soft tissues. Osteotomies were initiated following a palatally shifted trajectory, ensuring parallelism among implants and optimal distribution along the arch. Six straight MegaGen BlueDiamond® implants (diameters 3.3, 3.7, and 4.1 mm) were placed between the canine and first molar regions, avoiding sinus floor perforation and eliminating the need for sinus augmentation procedures.
Osseodensification Protocol Using Densah® Burs
Given the reduced bone density and limited ridge width in the maxilla, implant site preparation was performed using an osseodensification protocol with Densah® burs (Versah®, USA). Unlike conventional subtractive drilling, osseodensification is a nonextractive technique that preserves and compacts bone along the walls of the osteotomy.
The Densah® burs were used in a counterclockwise (densifying) mode at controlled speeds under copious irrigation. This technique promotes lateral compaction and autografting of bone particles into the trabecular spaces, increasing peri-implant bone density and enhancing the mechanical properties of the osteotomy site. In narrow ridges, osseodensification also allows controlled ridge expansion without fracturing the cortical plates, which is particularly advantageous in severely resorbed maxillae.
Scientific evidence has demonstrated that osseodensification increases insertion torque, improves bone-to-implant contact, and enhances primary stability, especially in lowdensity bone (D3–D4). In the present case, the use of Densah® burs was a critical factor in achieving high primary stability values, despite the compromised bone conditions.
Implant Placement and Primary Stability
All maxillary implants achieved insertion torque values exceeding 40 Ncm, confirming excellent primary stability and validating the combined use of a palatal approach and osseodensification. Implant platforms were positioned at bone level, with careful attention to prosthetic alignment and emergence.
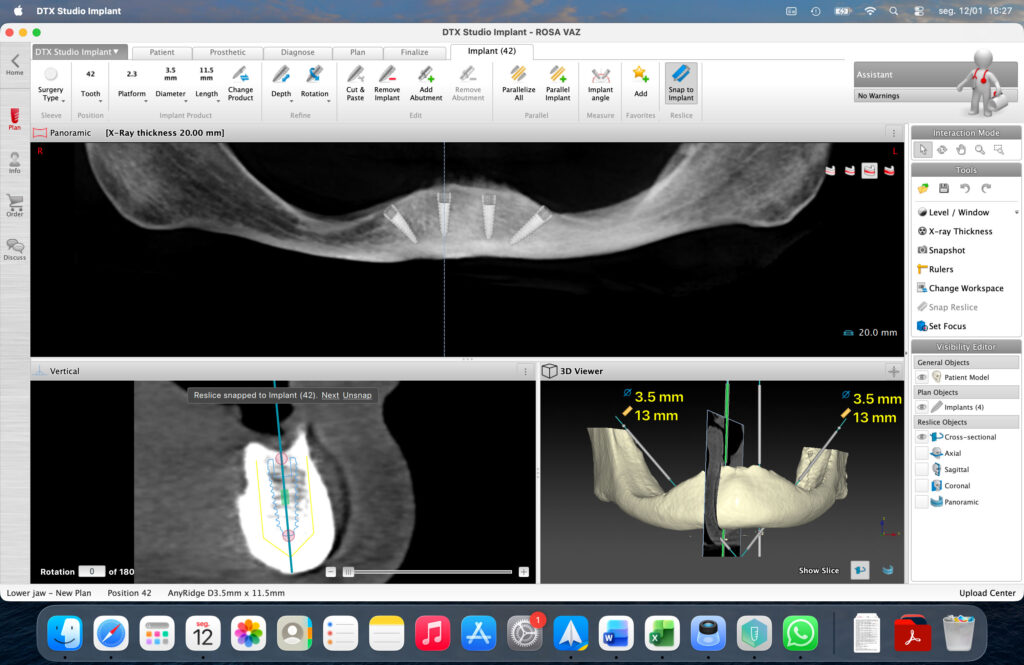
In the mandible, four MegaGen AnyRidge® implants (diameters 3.5 and 4.0 mm) were placed following an All-on-4 configuration. Posterior implants were tilted to avoid the inferior alveolar nerve and to maximize anteroposterior spread. All mandibular implants also achieved insertion torque values above 40 Ncm, allowing immediate or early loading considerations.
Post-surgical Considerations
The surgical sites were irrigated, and soft tissues were sutured with resorbable sutures to ensure tension-free closure. Postoperative instructions and pharmacological protocols were provided according to standard clinical guidelines. The patient experienced an uneventful healing period, with no signs of infection or neurosensory disturbances.


Prosthetic Rehabilitation
The provisional restorations were designed to minimize cantilever forces and provide balanced occlusion. After the osseointegration period, definitive fixed full-arch prostheses were fabricated and delivered.
Outcome and Follow-Up




Postoperative healing was uneventful. Radiographic follow-up demonstrated stable crestal bone levels around all implants. The patient reported significant improvement in comfort, masticatory efficiency, and quality of life.
Discussion
Osseodensification has been extensively studied as a method to improve implant stability in low-density bone. Unlike conventional drilling, which removes bone, osseodensification compacts trabecular bone outward, increasing peri-implant bone density and potentially enhancing secondary stability through improved bone remodeling.
Several experimental and clinical studies have demonstrated increased insertion torque, higher implant stability quotient (ISQ) values, and improved bone-to-implant contact when using Densah® burs, particularly in the posterior maxilla. These advantages are especially relevant in full-arch immediate-loading protocols where primary stability is critical.
The combination of osseodensification and implants with aggressive macrogeometry, such as MegaGen BlueDiamond® and AnyRidge®, provides a synergistic approach to managing severely atrophic jaws without resorting to extensive regenerative procedures.
Conclusion
This clinical case report highlights the feasibility of full-arch implant rehabilitation in severely compromised anatomical conditions through a carefully selected surgical approach. In the maxilla, the placement of six straight MegaGen BlueDiamond® implants following an All-on-Six protocol, combined with a palatal approach, allowed engagement of denser palatal cortical bone and avoidance of buccal bone dehiscence in the presence of advanced ridge atrophy, Kelly syndrome, and pronounced sinus pneumatization.
The use of osseodensification with Densah® burs proved to be a decisive factor in enhancing primary stability in low-density maxillary bone. By preserving and compacting bone during osteotomy preparation, this technique enabled insertion torque values exceeding 40 Ncm in all implants, despite limited bone height and width. This approach reduced the need for additional regenerative procedures, thereby minimizing surgical morbidity.
In the mandible, rehabilitation with an All-on-4 protocol using MegaGen AnyRidge® implants allowed safe implant placement while respecting the anterior position of the inferior alveolar nerve. Tilting of the posterior implants provided adequate anteroposterior spread and favorable biomechanical conditions without neurosensory complications.
Within the limitations inherent to a single case report, the combined use of a palatal approach and osseodensification appears to be a biologically sound and clinically effective strategy for the rehabilitation of atrophic jaws. Further prospective studies and long-term clinical data are required to confirm the reproducibility and longevity of these outcomes.
References
- Huwais S, Meyer EG. A novel osseous densification approach in implant osteotomy preparation to increase primary stability, bone mineral density, and bone-to-implant contact. Int J Oral Maxillofac Implants. 2017;32(1):27–36.
- Trisi P, Berardini M, Falco A, Vulpiani MP. New osseodensification implant site preparation method to increase bone density in low-density bone: in vivo evaluation in sheep. Implant Dent. 2016;25(1):24–31.
- Lahens B, Neiva R, Tovar N, et al. Biomechanical and histologic basis of osseodensification drilling for endosteal implants in low-density bone: an experimental study in sheep. J Mech Behav Biomed Mater. 2016;63:56–65.
- Misch CE. Dental implant prosthetics. 2nd ed. St. Louis: Mosby Elsevier; 2015.
- Malo P, Rangert B, Nobre M. All-on-4 immediate-function concept with Brånemark system implants for completely edentulous mandibles: a retrospective clinical study. Clin Implant Dent Relat Res. 2003;5(Suppl 1):2–9.
- Agliardi E, Panigatti S, Clericò M, Villa C, Malo P. Immediate rehabilitation of the edentulous jaws with full fixed prostheses supported by four implants: interim results of a single cohort prospective study. Clin Oral Implants Res.2010;21(5):459–465.
- Jensen OT, Adams MW, Cottam JR. All-on-4 treatment concept: biomechanical and clinical considerations. J Oral Maxillofac Surg. 2014;72(11):2194–2204.
- Sclar AG. Soft tissue and esthetic considerations in implant therapy. Chicago: Quintessence Publishing; 2003.
- Tolstunov L, Hicke B. Horizontal bone deficiency in implant dentistry: management and decision-making. J Oral Implantol. 2013;39(2):145–155.
- Esposito M, Grusovin MG, Rees J, et al. Effectiveness of sinus lift procedures for dental implant rehabilitation: a Cochrane systematic review. Eur J Oral Implantol. 2010;3(1):7–26.

Professional Bio
Dr. José Afonso Teixeira is a Portuguese dental surgeon and implantologist with over 21 years of clinical experience in oral surgery and advanced implantology. He is the Clinical Director of SorrisOeste – Clínica Médica and Clinica do Chapim and has extensive expertise in complex implant rehabilitation, including immediate loading, full-arch restorations, zygomatic implants, and advanced bone regeneration techniques. Dr. Teixeira has served as an international lecturer and clinical trainer in implantology, collaborating with leading implant companies such as Nobel Biocare and DIO Implants, where he has trained dentists in guided and navigated implant surgery. His clinical work focuses on advanced surgical protocols, digital implant planning, and minimally invasive techniques for complex cases. He holds a Master’s degree in Esthetic Implantology, Regeneration, and Advanced Periodontology (DEIPA – UCAM / NYU) and has completed numerous advanced training programs in implant surgery and regenerative techniques. Dr. Teixeira regularly participates in international congresses and educational programs, sharing his experience in modern implant rehabilitation and surgical innovation.